Let's open this posting with some background information. Since it is important to help put this information into context, let's look at the PULS Cardiac Test as shown here:
PULS (Protein Unstable Lesion Signature) is a blood test that is used to measure protein biomarkers that measure the body's immune system response to arterial injuries. Unstable lesions begin to form when damaged lipids bind to the interior surface of an artery, resulting in injury to that part of the artery. It is these injuries that form on the walls of the bodies arteries which lead to the progressive formation of cardiac lesions which can rupture and lead to a cardiac event.
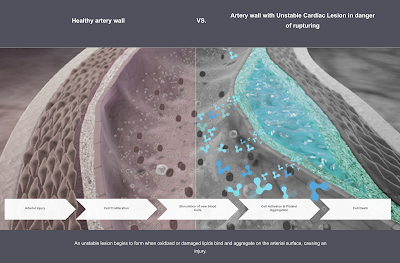
Here is a graphic showing a healthy arterial wall in comparison to an arterial wall with a lesion:
The PULS Cardiac Test is a serum blood test which identifies those asymptomatic patients which are at risk for Acute Coronary Syndrome (i.e. heart attacks, angina etcetera) by quantifying damage to the interior membranes of the heart and blood vessels (endothelium). Here is what the PULS test does:
"The PULS Cardiac Test quantifies 9 clinically-significant protein biomarkers that are activated by the body’s immune response to endothelial damage. These measurements are calculated into a single score that predicts ACS in a 5-year time frame."
In other words, the PULS Cardiac Test allows physicians to determine a patient's risk (percentage chance) of the occurrence of an Acute Coronary Syndrome over a five year period. This is key because the rupture of unstable cardiac lesions causes 75 percent of all heart attacks.
A recent abstract which appeared on the American Heart Association's Circulation website looks at how the PULS test is being used in conjunction with the administration of the mRNA vaccines that are being used to save the world from the SARS-CoV-2 virus. The author of the study, Dr. Steven R. Gundry, a cardiologist and researcher, has used the PULS Cardiac Test to follow 566 of his patients for the past 8 years, administering the PULS test every three to six months. The patients in the study range in age from 28 to 97 years and have a male to female ratio of one to one. He administered a new PULS test to this patient group from two to ten weeks following the patients' second COVID-19 mRNA vaccination and compared this result to the PULS score drawn from tests administered three to five months prior to the vaccination.
Here's what he found
1.) PULS Score - the PLUS score increased from an 11 percent risk of an ACS over the next five years to a 25 percent risk of an ACS over the next five years, an increase of 14 percentage points or a 127.3 percent increase.
2.) The changes to the PLUS score persisted for at least 2.5 months after the second dose of the COVID-19 mRNA vaccine.
Dr. Gundry concluded the following:
"...the mRNA vaccines dramatically increase inflammation on the endothelium as well as increasing the T cell infiltration of (T cells or T lymphocytes are part of the body's immune system) which may account for the observations of increased thrombosis, cardiomyopathy and other vascular events following vaccination."
Since research that does not particularly paint the COVID-19 vaccines in a positive light tends to disappear from the internet, here is a screen capture of the entire abstract:

While the general public does not have access to the entire study, the abstract provides us with information that may explain this:
....and this:





I would be curious if you've ever looked at the stats on existing vaccines. The old saying goes that nothing's perfect, so I have to assume there are incidences of things going wrong. What would the percentage of problems be with existing vaccines? How does that compare to the questions you're raising about mRNA? Is there some sort of "norm" of bad with any good?
ReplyDeleteBy the way, were you aware of existing vaccine requirements? Government of Ontario web site: Vaccines for children at school. Can I interpret that as a "vaccine mandate"? I asked my niece, a high school teacher, about this, and while she's aware of this rule, she's not sure it's implemented 100%.
WQB
ReplyDeleteHere is interesting research from two researchers about the mRNA vaccines:
https://doctors4covidethics.org/on-covid-vaccines-why-they-cannot-work-and-irrefutable-evidence-of-their-causative-role-in-deaths-after-vaccination/
I am a layperson and do not pretend to understand the scientific details of the paper you mentioned or the following rebuttal. As I previously said to you, I'll be interested to see what expert analysis concludes sometime in the future, let's say five years, of what was good and what was bad about our pandemic response.
ReplyDeleteClaim:
On COVID vaccines: why they cannot work, and irrefutable evidence of their causative role in deaths after vaccination by Sucharit Bhakdi, MD and Arne Burkhardt, MD
Rebuttal:
Fact Check-A four-page, yet to be peer-reviewed paper is not proof that COVID-19 vaccines cause 93% of deaths that occur after inoculation, Reuters Fact Check, Jan 7/2022
We have to be careful when using Reuters. The President, CEO and Director of Reuters, James C Smith, just happens to be on the Board of Directors of Pfizer. Do you think that he might just have a conflict of interest?
ReplyDeletehttps://www.pfizer.com/people/leadership/board_of_directors/james_smith
This is why it is so damnably hard to cipher out the truth in the post-truth era. Everyone has an agenda. A significant part of the mainstream media is also funded by Bill Gates through the BMGF so, obviously, they are hardly trustworthy.